- Joined
- Jun 15, 2026
- Posts
- 7
- Reaction score
- 19
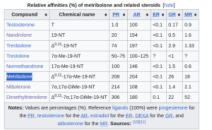
Metribolone a/k/a 17a-Methyltrienolone (17β-hydroxy-17α-methyl-estra-4,9,11-trien-3-one)
» What is Metribolone (A/K/A MTren)?
Metribolone is a syntethic steroid, precisely its the 17α-methylated derative of Trenbolone (hence the name 17a-Methyltrienolone), now on the surface it may look like its just the oral version of trenbolone, WRONG! The compound was first characterized in the mid-1970s by Bonne & Raynaud, who showed it binds to the rat prostate androgen receptor with roughly twice the affinity of DHT, a Kd of 0.6 nM versus 1.4 nM for DHT [1] [2].
Glucocorticoid receptor: Ho-Kim et al. [3] showed that in rat muscle cytosol, R1881 binds to glucocorticoid receptors (GR) too. After adrenalectomy, [³H]R1881 binding doubled compared to [³H]testosterone, and competition experiments confirmed that R1881 competes for triamcinolone acetonide binding sites on GR. If you believed Trenbolone had a strong affinity for GR, youre mistaken:
Mineralocorticoid receptor: Takeda et al. [4] demonstrated that it binds the mineralocorticoid receptor (MR) with the same affinity as aldosterone itself, an apparent Kd of ~0.75 nM vs 0.5 nM for aldosterone jfl. And unlike aldosterone, R1881 does not activate MR, it acts as a potent MR antagonist.
Progesterone receptor: Asselin et al. [5] found that in human benign prostatic hypertrophy tissue, R1881 binds just as well to progesterone receptor (PgR) as it does to the androgen receptor. Progesterone and the synthetic progestin R5020 potently compete for R1881 binding in that tissue.
» What about the risks associated with the use of it?
Due to it having a 17a-alkylated chemical structure, resistance to hepatic metabolism, and the downstream induction of oxidative stress and mitochondrial dysfunction in hepatocytes. In a early study, Krüskemper [6] demonstrated that methyltrienolone caused biochemical signs of intrahepatic cholestasis at extremely low doses (0.1–1.0 mg/day) BUT it was mostly done using the oral version and in sick females and males. Plus all the normal sides from 19-nors/AAS.
» What is the best way to use it?
Firstly, we are gonna use an injectable version of it, if you're new to the community you may be wondering how an oral steroid can be formulated in a injectable form, well tldr is that the raw powder of the oral is dissolved in solvents and cosolvents then in oil base or water base.
Taking oral and taking injectable is drastically different, when you take 1mg oral, that milligram nvkes your liver at once, that puts immense load on the liver because it has a rate at which it metabolizes toxins, everything thats above that rate causes what we consider as liver damage, your liver is literally built to handle toxins, handling toxins is no problem, its when you exceed its metabolic rate that the left over toxins have time to damage your liver.
in all anecdotes on forums we see 2 groups of mtren users, mild elevation or severe elevation of liver enzymes, coincidentally it always boils down to oral or injectable usage. when using injectable, the metribolone disperses its way through your bloodstream, binding to androgen receptors, which means very little metribolone is left over for your liver to handle, which it does easily, remember, its built for toxins. yes, over the day its cummatively still 1mg of mtren, but the delivery to the liver is drastically dispersed instead of a big assault on the liver.
Lastly, because metribolone's higher molar mass and dosing in micrograms, it drastically drastically less molecules in the blood, so there is way less accummiliation in the brain compared to conventional tren.
» How are we gonna dose it?
Based on several studies, we can come to the conclusion that 500-750mcg of injectable methyltrenbolone provides full AR occupancy, pair it with a few ancilleries and you can run it prettty safe without getting much sides:
NOTE: I think that injecting it intramuscular (IM) is far better than subq because IM floods your plasma levels, if you get an erection after you pin it youre gonna have around 70x in your penis acting on the ARs there.
Liver
1g tudca split x 4
300mg na r ala split x 2
500mg nacet split x 2
10g taurine
1g silmaryin extract
Misc
25mcg T3
100mcg T4
Cardiovascular
80mg Telmisartan (ONLY IF YOUR BLOOD PREASSURE IS ELEVATED, IT INHIBTS TGF-B)
5-10mg Nebivolol (depending on rHR)
5-10mg Ezetimibe
10mg Rosuvastatin
Sleep
5-10mg Lemborexant
1mg Melatonin
1g tudca split x 4
300mg na r ala split x 2
500mg nacet split x 2
10g taurine
1g silmaryin extract
Misc
25mcg T3
100mcg T4
Cardiovascular
80mg Telmisartan (ONLY IF YOUR BLOOD PREASSURE IS ELEVATED, IT INHIBTS TGF-B)
5-10mg Nebivolol (depending on rHR)
5-10mg Ezetimibe
10mg Rosuvastatin
Sleep
5-10mg Lemborexant
1mg Melatonin
I reccomand cycling mtren 5-6 weeks on and then 5-6 weeks off, in the off period you could complement by running a different 19-nor such as NPP or Trenbolone.
Thanks for reading my thread
If you have any suggestions, points, studies, information you wanna point out feel free to reply to this and i'll check everything out.
If you have any suggestions, points, studies, information you wanna point out feel free to reply to this and i'll check everything out.